https://www.canadiancovidcarealliance.org/
https://www.skirsch.io/how-to-treat-covid/
This article primarily covers treating COVID, long-haul COVID, and side-effects from COVID vaccines. We also talk about the Together trial results, why clinical trials fail, etc. We include COVID prophylaxis and early treatments that do not currently require a prescription because in many countries the prescription drugs may not be available.
Disclaimer: This info is for educational purposes only. Please consult with your doctor before taking any drugs.
If you have to get a vaccine, which one is the safest?
Pfizer, then Moderna, then J&J. See Vaccine risk benefit by age.
How to avoid vaccine side effects
- Many people will try to get Sinovac-CoronaVac or Sinopharm. The vaccine doesn't work, but there are no side effects and you get your vaccine card which is the important thing. But it may not be "usable" in other countries.
- If you are forced to get one of the US vaccines, using .2mg/kg of ivermectin the day before, the day of, and the day after will reduce your chance of side effects by 95% according to a prominent researcher in Brazil we know. Of course, the FDA and AMA are trying their best to block your access to ivermectin, a new low for medicine. The mainstream medical community are cheering them on.
Treating COVID
Got COVID? Treating it ASAP is key for best outcomes. Even if it seems mild at first, treat COVID like you'd treat a fire in your house: the sooner you put it out, the less the long term damage.
Remember: The only thing all the COVID patients in hospitals today have in common today is that they didn't treat their infection using a proven early treatment protocol (or they waited too long).
Step 1: Find a doc, get a prescription, and get the medications filled now so that they can be on hand for your immediate use. This is critical for new variants because every hour counts. In some cases, you may need to have another condition in order to get a prescription, e.g., if you have OCD, you can get fluvoxamine for that condition and the use for COVID is a nice fringe benefit. There are also some treatments that don't require a prescription.
Step 2: As soon as you think you might have COVID, start treatment. Don't wait for a positive test. If your test result ends up being negative, stop the treatment. Because the treatments are so safe, everyone, even kids, can and should be treated immediately upon suspected COVID. Early treatment reduces risk of hospitalization, death, and reduces the chance of getting long-haul COVID which can be very hard to treat. If you started treatment early, your symptoms should start reversing about 24 hours after you start treatment.
List of doctors
Your doctor is unlikely to know how to treat you correctly. Here is a list of telemedicine providers who know their stuff and will give you a prescription for you to fill now so that you will have ALL the drugs on hand if/when you get sick. This is important because you want to have all the drugs immediately available. Time is critical.
List of doctors who will write early treatment COVID prescriptions
They generally will prescribe to you one of the following early treatment protocols or some modification that they personally like. Each physician ends up using his own judgement based on what they've personally seen work the best.
- Modified Patterson protocol (shown below)
- I-MASK+ protocol from flccc.net. See this Chris Martenson video.
- Tyson-Fareed protocol: Has 99.76% risk reduction and no safety downsides.
- Zelenko early treatment protocol: Another highly effective treatment.
- Chetty protocol: Described in this paper, it has over 99% risk reduction.
- Italy protocol: This is extremely effective. Reportedly, only 4 out of 66,000 people died in Italy. This is an HCQ-based protocol because ivermectin is prohibited in Italy.
- Egyptian protocol: Very successful in Egypt
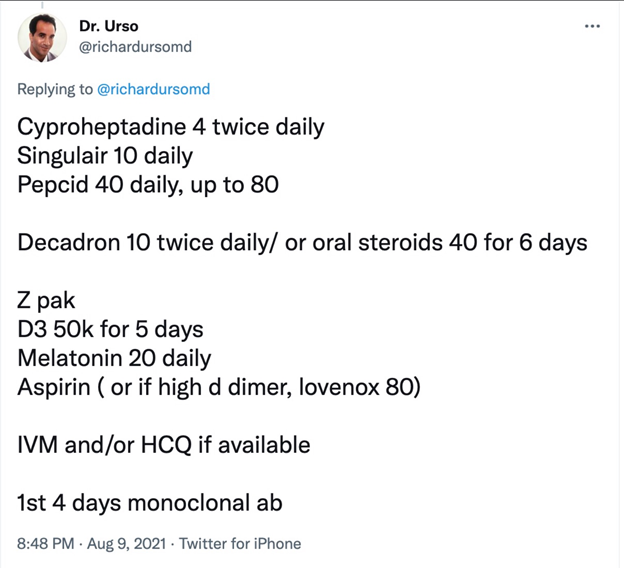
- Dr. Urso protocol (the lack of units is a bit troubling):
Modified Patterson early treatment protocol for COVID
Based on recommendation of Dr. Bruce Patterson with a few minor improvements. Patterson who treats thousands of long-haul COVID and vaccine cases so he knowns more than anyone else the drugs that in combination are the most effective in countering the inflammation caused by COVID. Take all drugs (that you can access) IMMEDIATELY after you suspect a COVID infection (except as indicated). The following are all safe and do not interact with each other.
- Fluvoxamine (luvox) 50mg twice a day for 14day. If not available, use fluoxetine (prozac) 30mg once a day x 14 days. If already on an antidepressant, consider talking to your doctor about switching. Avoid caffeine, alcohol, tylenol, and benadryl while on fluvoxamine. Fluvoxamine prevents brain fog because it passes through the blood brain barrier. In rare cases, can cause hair loss. If you can't tolerate fluvoxamine, try Prozac instead. It works just as well (proven in multiple observational studies). If you are jittery, have dilated pupils, or other side effects, you may need to reduce the dosage. For details on fluvoxamine, see My substack article on fluvoxamine.
- Ivermectin .4 mg/kg every day for a minimum of 10 days and continue until symptoms resolved. Take with a meal or right after a meal for best absorption. Ivermectin is one of the safest drugs ever invented. See the FLCCC website for more info. Some people are super sensitive and can't take that dose every day. In that case, taking it every 3 days should be fine since it is slowly eliminated from your body.
- Inhaled budesonide: 400 µg per actuation (two puffs to be taken twice per day; total dose per day 1600 µg) x 14 days (or until resolution of respiratory symptoms). You really want to throw the kitchen sink at this virus and the number one reason people got to the hospital is respiratory distress. The latest Together trial will be testing fluvoxamine and budesonide in combination. We recommend this even if you don't appear to have any respiratory symptoms because you want to play it safe and keep it that way.
- NAC: 600mg/day for 14 days. This mitigates the damage caused by the spike protein. This is a super safe drug that was available over the counter for 60 years. After 60 years of safety, and incorporation in 1,500 products, it was made prescription only so people would not have access to it and would be forced to get vaccinated.
- Vitamin D3: 15,000 IU/day for 14 days to lower inflammation.
- Pravastatin: 20mg x 14 days. Other statins can be used but this is the best.
Early-treatment "options"
Here are a few optional "add-ons" that you can safely add to any of the protocols that can make a difference (if not already in your protocol). You can even do quite well using these as your only defense. Although all are available without a prescription, always discuss with your doctor before taking these. They can be considered if you cannot adopt a proven combo protocol or you simply want an extra margin of protection.
It is not always the case that more is better. You can run into weird interactions when taking lots of drugs at the same time.
- Benadryl + lactoferrin: Take as soon as you have symptoms. Both are very safe and available without a prescription. Together they are 99% effective according to this article. Here is the paper. CAUTION: Do not combine benadryl and fluvoxamine; they interact. Benadryl can cause your eyes to dilate.
- Aspirin: Reduces chance of death by around 50%. Either size works. Take once a day for 10 days after first symptoms.
- Nigella sativa (no prescription needed)
Black seeds 40mg/kg orally once per day for 14 days. $9 gets you a 70 day supply. Reduces hospitalization risk by 75%. Death by 95% . - Vitamin D3: 15,000 IU/day for 14 days to lower inflammation. Up to 80% reduced risk. Ideally, you'll want to take with magnesium for complete absorption. Also, if you try to load up AFTER you get COVID, it will take too long unless you pre-order this and have it on hand: d.velop Vitamin D.
- Povidone-iodine (Betadine): .5% to 1% solution (no prescription needed; widely available at drug stores at low cost). Do it 3 times a day for the first 3 days. The 1% will be somewhat uncomfortable. The .5% will hurt less. So if you can't tolerate the 1%, dilute it down 1:1 with purified water.
The pro tip is to buy the 10% solution and then dilute it down to 1% or even .5%. Otherwise you'll be sorry. So a bottle of the 10% solution (which will cost you around $15 or less for an 8oz container) is going to last you a LONG LONG time.
Mouthwash/gargle and nasal drops (or rinse) 3 times a day starting on first symptoms. After 7 days you'll see a 99% drop in viral load and you'll lower your risk of death by nearly 90%. See Effect of 1% Povidone Iodine Mouthwash/Gargle, Nasal and Eye Drop in COVID-19 patients and Rapid initiation of nasal saline irrigation: hospitalizations in COVID-19 patients randomized to alkalinization or povidone-iodine compared to a national dataset which shows that early treatment can reduce your risk by 95% if you start early for just this one simple, easy, very safe intervention. You can get both solutions on Amazon or at www.immunemist.com. DO NOT USE THIS EVERYDAY as a prophylaxis. Instead, use within 12 hours of higher risk contact, or twice a day for 14 days if you get infected with COVID. It's basically a stronger solution than the hypertonic saline solution. - Colgate Total (no prescription needed)
Total contains cetyl pyridinium chloride (CPC). Within 12 hours after possible contact, swish and gargle for 30 seconds and put a saturated Qtip up your nose (watch this instructional video). You can use other mouthwashes with CPC. This is a very simple and inexpensive solution to the problem ($5 per month) that protects you against other viruses as well. - Hypertonic saline solution nasal rinse (no prescription needed)
Create a hypertonic solution by adding 1 tsp of salt (5g) to 8oz water. This will create a 2% solution. Do a nasal rinse with a squeeze bottle (I use the 8 oz NeilMed squeeze bottle) or a neti pot. If you do the rinses occasionally (because you are rarely exposed), the NeilMed bottle is fine. If you do more often, the neti pot is better since there is no pressure so less potential damage to sensitive nasal structures. Do this within 12 hours after a risky incident (e.g., before bed). For extra credit, with remaining hypertonic solution, gargle, swish and then spit after 20-30 seconds. However, most COVID infections are through the nose. A lot of doctors say you should use purified or distilled water. Others I highly respect say that's overkill and say tap water is fine. I've always used warm tap water (at same temperature as your body temperature) and never had a problem. Compliance is the most important factor. - NAC: 600mg/day for 14 days. This mitigates the damage caused by the spike protein. This is a super safe drug that was available over the counter for 60 years. After 60 years of safety, and incorporation in 1,500 products, it was made prescription only so people would not have access to it and would be forced to get vaccinated. I bought mine at Thorne. No prescription needed.
- Glutamine: 10 g l-Glutamine available in powder forms were given 3 times a day with meals. In the control group, 38 out of 230 covid patients died. In the glutamine group, 0 out of 222 patients died:The effect of glutamine supplementation on serum levels of some inflammatory factors, oxidative stress, and appetite in COVID-19 patients: a case-control study - PubMed (nih.gov) Again, no mortality and no ICU admission in the glutamine group… Effect of oral l-Glutamine supplementation on Covid-19 treatment - PubMed (nih.gov)
Prophylaxis protocols (recommended)
Lactoferrin (no prescription needed)
"“We found lactoferrin had remarkable efficacy for preventing infection, working better than anything else we observed," Sexton said. He adds that early data suggest this efficacy extends even to newer variants of SARS-CoV2, including the highly transmissible Delta variant.” This is safe.
However, it may be more convenient just to skip the prophylaxis, get COVID, and treat it early.
Prophylaxis protocols (not recommended)
FLCCC prophylaxis protocol
This is an ivermectin-based protocol. However, in consultation with other docs (gut specialists), I do not recommend it because it will destroy the good bacteria in your gut. In general, do not take prescription drugs for prophylaxis.
Nasal irrigation (no prescription needed)
Done twice a day has been remarkably effective in preventing COVID infections. See hypertonic above for details. Again, this is NOT recommended because you will upset the bacteria balance in your nose. If you do it, you only want to treat on an acute basis (i.e., when you are sick).
Other drugs that work against COVID-19
See C19 Early for a list of drugs and effect sizes.
Treating long haul COVID
Bruce Patterson’s long haul COVID treatment relies on four drugs. The dosing depends on what your bloodwork shows (based on the Cytokine 14 panel available at covidlonghaulers.com), so the dosages are averages.
- Fluvoxamine: 50mg BID
- Ivermectin: .2mg/kg every 3 days
- Pravastatin: 20mg (substitute for fractal kinase inhibitor)
- Maraviroc 300mg PO BID. This reduces CCR5 and takes about 5 days to work.
The other option is going to covidlonghaulers.com and getting tested. Then they'll prescribe drugs based on your test results.
Treating pre- and Post-Vaccine Inflammatory Syndrome (PVIS)
Ideally start this 3 days before you vaccinate. Less ideally, start this immediately after vaccination.
Continue for 14 days if using to minimize vaccine side effects.
The longer you wait, the more likelihood of permanent damage to heart, lungs, and brain. Once those tissues are scarred from inflammation, they will never heal. This is why many long-haulers never regain full function. It's exactly the same story with vaccine victims. Watch this 8 minute video featuring Dr. Charles Hoffe.
- Fluvoxamine: 50mg BID (can substitute 30mg Prozac QD)
- Ivermectin: .2mg/kg daily. You may see results in less than 24 hours. Note this is a lower dose than an active COVID infection.
- Prednisone: 5mg/day for inflammation. Note: this is a low amount because if you give more you start to affect the immune system which is problematic because you want the macrophages to clear out the spike protein
- Pravastatin: 20mg (substitute for fractal kinase inhibitor)
- Maraviroc 300mg PO BID. This reduces CCR5 and takes about 5 days to work.
For best results, go to covidlonghaulers.com and getting tested with the 14 cytokine panel and they'll prescribe the appropriate drugs based on your test results (since the Maraviroc is pretty pricey). You also will want to get the Spike Protein test at incelldx.com (but it seems it isn't available as of Sept 7, 2021).
Or check out the FLCCC I-Recover protocol; it can be used for PVIS as well (as they note in the text).
Drugs that may be available in the future
These drugs will be difficult to impossible to obtain currently in the US but may be available in other countries:
- enovid. This drug is made by SaNOtize . It probably won't be available in your area, but it appears to be effective.
- Interferon Lambda: If you can get a single injection of Interferon Lambda (made by Eiger), that is the drug with the largest effect size and best safety profile. It is currently only available in clinical trials. It should be taken ASAP after infection for best results. It drastically reduces d-dimer which is an excellent indication that has a dramatic effect in lowering blood clotting (and likely inflammation). You basically will not get hospitalized if you get this drug. If you only can take one drug, this is the drug to take. If you can get access to this drug early, everything else is optional.
- Camostat: 200mg taken orally, 4 times daily, for 7 days will absolutely reduce your chance of long haul COVID symptoms and reduce your risk of hospitalization. It isn't approved in the US, but is approved in other countries. It will not change your time to recover. It's about preventing you from developing long-haul COVID symptoms and severe disease. It's an antiviral so take ASAP.
- Proxalutamide: Appears extremely impressive, near 100% efficacy. Now in Phase 3 trials in USA.
Currently, the five most effective drugs for COVID are:
- Interferon lambda
- Fluvoxamine or Fluoxetine (Prozac)
- Ivermectin
- Inhaled budesonide (see this tweet)
- Camostat
That list was made on July 26, 2021. It will be 4 months before the rest of the world figures it out.
Note about Together trial results for fluvoxamine and ivermectin
Why did Ivermectin seem to fail and Fluvoxamine not do so well? Ivermectin was dosed for 3 days; fluvoxamine for 10 days.
We don't think the trial was gamed at all. I think this was a legit result.
We know the PI Edward Mills and believe he is totally honest and we have no reason not to believe the results he obtained. But we also believe other researchers as well.
So the question everyone has is how could these drugs do so well in other studies?
The answer: the variant was different. P1 is the variant in Brazil and makes Delta look like a walk in the park. If you do not treat P1, instantly upon symptoms, you will see big failures.
Had fluvoxamine been given on Day 0 instead of Day 4, there would have been a dramatically different result.
Had ivermectin been dosed at .6mg/day for 14 days starting on Day 0 (the first day of symptoms), there would have been a dramatically different result.
The more aggressive the variant, the earlier and harder you have to treat it.
Ivermectin likely failed for these five reasons:
- Too little a dose
- Started too late
- Not taken with meal or shortly after
- Not continued for long enough
- Many patients may have already been taking ivermectin
The healthcare systems need to encourage people to have the meds in the cabinet for immediate use. Nobody does that. That's why we have a problem.
Also, you can't treat Delta and P1 in the hospital... it is much much tougher there. It's like a fire department arriving when the entire building is in flames.
Early aggressive treatment is key. There are near ZERO hospitalizations and DEATHs for anyone treated early. But the press never talks about that. The NIH or CDC never says that either. Why not?
You can't say vaccination works: at Mt Sinai in NY, 27% of the hospitalized cases are vaccinated, and 17% of ICU patients are vaccinated.
The sooner we stop following the NIH advice that early treatments don't work, the sooner we will start saving lives.
Ways a clinical trial can fail
Clinical trials on repurposed drugs should always be tested first on outpatients by physicians who prescribe on a shared decision making basis. Once a protocol is found to be reliable, then it can be "locked" into a clinical trial for "proof" of efficacy. Sadly, we do the opposite which wastes a lot of time and money. We form a hypothesis and then invest millions to test it out in a large scale trial rather than on an outpatient basis.
Here are some ways a clinical trial can fail.
- Dose: standard dosing may need to be increased for new variants. The FLV dosing of 50mg BID was tested for alpha variant. In general, increase dose for aggressive variants or treatment that is started later after infection. In this trial they used 100mg BID. The downside is that this dose can lead to compliance problems where people have to discontinue the use of the drug.
- Timing: Ivermectin is best taken with a fatty meal or right after, not on an empty stomach. The FDA however requires the drug to be taken on an empty stomach in trials due to worries about liver toxicity, even though this hasn't been a problem in any other trial. This seems very silly.
- Treatment delay: Treatment in Together started on average 4 days after symptoms. Too long of a wait especially for fast replicating variants like Delta. The lesson is start treatment IMMEDIATELY after symptoms recognized or before, especially with aggressively replicating variants. This is the most important determinants of success; once the damage is done, it is hard to reverse. This is the most important thing to get right.
- Compliance: Patient compliance in the Together trial was estimated to be somewhere around 80%. If compliance is low, it is going to limit your effect size. How can the study prove that everyone took all their meds as directed? We can only see this by looking at the source data of the study for clues. As the pandemic continues, we've found patient compliance to drop dramatically. Early in the pandemic, you could call participants and talk to you. Today, you call and they hang up on you.
- Duration: Delta can hang around for 33 days. Treatment should be continued until 5 days after symptoms resolve. So shouldn't be a fixed duration (like it was in the trial). In the trial, the duration for ivermectin was only 3 days; was 10 days for fluvoxamine.
- Deception: Participants were supposed to be early in COVID, but many could have given inaccurate information either willfully or mistakenly. There was no way to tell because this wasn't measured. This explains how so many ended up in the hospital so fast (e.g., within 1 day after treatment started). There wasn't baseline bloodwork taken to assess disease state of the participants. They could have determined disease stage from this and better assessed outcomes.
- Lack of adaptability: Some doctors find that using D-dimer and CRP to guide the dose and duration can be very helpful. That is rarely done in a clinical trial.
- Single drug: Using a multi-drug protocol will work better especially if the drugs are synergistic. For example, many people claim HCQ without zinc is a non-starter.
- Tampering: Phase 3 trials don't have levels of controls to detect manipulation. It relies on everyone being trustable in doing their jobs. If the drugs are switched accidentally (placebo vs. real drug), no one will know. This is why it is important to look at the source data and the side effect reports. Even the best designed studies are susceptible to tampering. That tampering could be deliberate or accidental and it can be hard to detect.
- Data manipulation: One ivermectin study showing a positive result was clearly manipulated. Data manipulation does happen. It can sometimes take months before this is exposed.
- Controls may already be taking one of the study drugs: A major reason why ivermectin trials don't fare too well in S. America is that lots of controls may have taken ivermectin. For example, in the TOGETHER trial, it was NOT an exclusion criteria (and so the data should be segmented by that before coming to conclusions).
- Dropouts. People can drop out of the trial causing you to lose statistical power.
- Missing data. People can not report back what happened.
- Low event rate. You may underpower the trial because people are healthier than you presumed or the virus mutates to a less dangerous strain.
- Competitive sabotage. A competitor can pay enrollees to enroll in the trial and not take the drug.
These are issues that can come up with any trials, even well done trials. It's a shame these trials in general do not have more controls to detect these mistakes. They happen. This is a known limitation of every clinical trial; few if any have any robustness to errors.
One other very important point is that researchers are PROHIBITED by their IRB and other entities from testing ivermectin doses and durations that would be effective! One doctor in the US just told me that they wouldn't let him go higher than 200mg/kg for 3 days. That's crazy. Ivermectin is one of the safest drugs on the planet.
An idea for rapidly screening drugs against COVID
The biggest problem with COVID is the inflammation and clotting. The vaccines create the same rise in CRP and D-dimer as COVID and it's very reliable (happens post-vax in over 60% of cases).
Therefore, if we want to test a single drug against COVID, all we need is 5 volunteers who have been recently vaccinated. Treat immediately after vaccination with the drug. Measure CRP and D-dimer at 5 days. If both are normal in all 5 patients in 5 days, you have a candidate drug.
Once you have 3 candidate drugs and test the combo in a clinical trial.
For more information
- Early treatment is key to better outcomes
- Detailed advice on treatment
- Ten things to know about treating COVID infections
- Drugs and dosages
- Summary of what we know about treating early (just read the introduction)
- Short summary of the case for using fluvoxamine for COVID (slides only)
- Video presentation of the slides: 15 minutes at start of Semmelweis effect seminar
- Detailed summary of the evidence supporting the use of fluvoxamine for COVID
The tl;dr is that every piece of evidence we have ever seen (observational studies, randomized trials, doctor experiences) is positive. There are no cases where fluvoxamine made things worse. If treated early enough with fluvoxamine, patients can recover and completely avoid long-haul COVID issues. - COVID-19 Early Treatment Fund (CETF) Introduction - YouTube
- Fluvoxamine: Finding a possible early treatment for COVID-19 in a 40-year-old antidepressant - 60 Minutes - CBS News
https://americanbuddhist.net/2021/12/13/france-covid-mortality-with-vs-without-hcq/
In a recent presentation, Pr. Million from IHU Marseille has presented their first numbers of Covid mortality by age group in 2021.
He has highlighted the improved 2021 mortality where patients did not get HCQ+AZ, which he attributed to the discreet introduction of Ivermectin.

IHU has adopted Ivermectin in 2021 but has stayed silent about it.
Possibly to avoid controversy and maintain access to the drug, and more likely because French regulators insisted that off-label use was a right but any publicity would be sanctioned.